
12 Lead ECG Placement: A Step-by-Step Guide

The 12 lead ECG is a crucial diagnostic tool for assessing heart function. Proper placement of electrodes is essential for accurate readings and effective diagnosis. Various leads provide insights into different areas of the heart. Understanding the correct placement techniques can enhance the quality of the ECG results.
The system uses specific leads to detect the heart’s electrical activity from various angles. Each lead provides a unique view, contributing to a comprehensive analysis of heart function. After attaching all leads, ensure they are securely connected to the ECG machine to check for any loose connections or interference. With the patient still and relaxed, start the ECG and monitor the initial readings for any abnormalities or artifacts. After completing the ECG, gently remove the electrodes, clean the skin, and document the procedure correctly.
Patient Preparation for a 12 Lead ECG
Before placing electrodes, proper preparation is essential for accurate tracings and to reduce artifacts:
- Explain the procedure and obtain informed consent where required.
- Position the patient lying supine or semi‑recumbent, with arms and legs relaxed and uncrossed.
- Ensure the room is comfortably warm to avoid shivering and muscle tension.
- Clean the skin with soap and water or alcohol wipes if oily, and dry thoroughly.
- Clip or shave excessive chest hair at electrode sites to improve contact.
- Remove or reposition jewelry, phones, and electronic devices that may interfere.
Proper skin preparation and patient positioning help reduce motion artefact and baseline wander, improving ECG interpretation.
Standard Limb Lead Placement for a Resting 12 Lead ECG
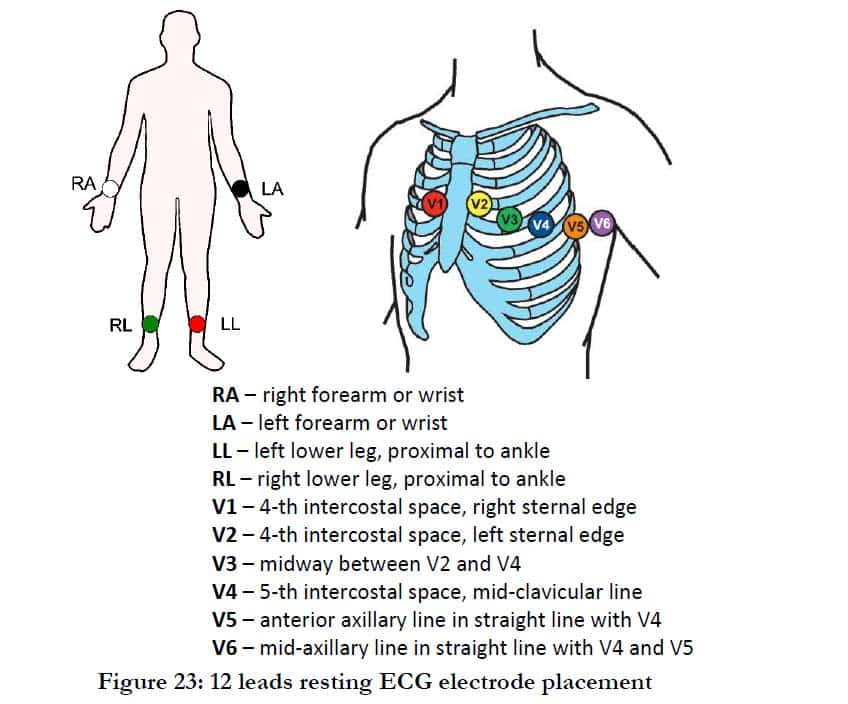
In a standard resting 12 lead ECG, limb electrodes are placed on the arms and legs rather than on the torso. Use the following positions:
- RA (Right Arm): On the right arm between the shoulder and elbow, distal to the axillary fold.
- LA (Left Arm): On the left arm between the shoulder and elbow, distal to the axillary fold.
- RL (Right Leg): On the right leg below the torso and above the ankle, anywhere on the leg.
- LL (Left Leg): On the left leg below the torso and above the ankle, anywhere on the leg.
These four electrodes generate the six frontal plane leads: I, II, III, aVR, aVL, and aVF. For exercise tests or specific protocols, Mason–Likar torso positions may be used, but for standard diagnostic resting ECG, limb electrodes must remain on the limbs.
Chest Lead Placement V1–V6 in Adults
Correct chest lead placement requires identifying intercostal spaces and anatomical landmarks. Use this step‑by‑step approach:
- V1: Fourth intercostal space at the right sternal border.
- V2: Fourth intercostal space at the left sternal border.
- V4: Fifth intercostal space at the mid‑clavicular line on the left side.
- V3: Midway between V2 and V4 along a straight line.
- V5: Left anterior axillary line at the same horizontal level as V4.
- V6: Left mid‑axillary line at the same horizontal level as V4 and V5.
V4, V5, and V6 must line up horizontally in the fifth intercostal space; placing them too high or too low can significantly alter ST segments and QRS morphology. For female patients, place V4–V6 under the breast tissue following anatomical landmarks; do not use the nipple as a reference point.
12 Lead ECG placement (video guide)
Watch the following technical video demonstration to verify proper connection and placement procedures:
What is a 12 Lead ECG?
A standard 12 lead electrocardiogram (ECG) records the heart’s electrical activity from 12 different views using 10 electrodes placed on the limbs and chest. These 12 leads capture electrical signals in the frontal plane (limb leads) and horizontal plane (chest leads), helping clinicians detect rhythm disturbances, ischemia, conduction abnormalities, and previous myocardial infarction. A 12 lead ECG is routinely used in emergency departments, cardiology clinics, ambulance services, and pre‑operative assessments as a non‑invasive diagnostic test.
Typical reasons to perform a 12 lead ECG include chest pain or pressure suggestive of acute coronary syndrome, palpitations, irregular heartbeat, suspected arrhythmias, syncope, dizziness, or unexplained episodes of collapse. It is also standard for pre‑operative cardiovascular assessments or monitoring patients with known heart disease. Always document the indication, time of recording, and clinical context in the patient record.
Why Are There Only 10 Leads in a 12 Lead ECG Placement?
Although it’s referred to as the 12 Lead placement, an ECG only uses ten electrodes for reading. Some electrodes form a pair, which provides this tool with two Leads. The electrodes are self-sticking pads containing a conducting gel at their centers. On the other side, the electrodes snap onto the ECG’s or heart monitor’s connected cables.
The ECG shows a glimpse of the electrical activity taking place inside the heart, and does this from a particular angle. In layman’s terms, this method of medical investigation reads perspectives. Therefore, the ten electrodes in the 12 Lead EKG give 12 perspectives of the heart’s electrical activity at a given time, using various angles. This is all done via two electrical planes called the horizontal and vertical planes.
Pediatric 12 Lead ECG Placement
In children, the principles of electrode placement are similar, but anatomical proportions and clinical indications differ. Position the child supine or semi‑recumbent with a calm, warm environment to minimize movement. Use age‑appropriate explanations and, when possible, involve caregivers to reassure the child. Limb leads (RA, LA, RL, LL) are still applied to the arms and legs, adjusting for smaller limb size. Chest leads V1–V6 follow the same intercostal landmarks, using gentle palpation to identify ribs. ECG interpretation in pediatrics requires specific training, as normal pediatric ECGs differ from adult patterns; always refer tracings to clinicians experienced in pediatric cardiology.
Common ECG Lead Placement Errors and How to Avoid Them
Lead misplacement can cause significant diagnostic errors, including false ST elevation or depression, apparent axis changes, and pseudo‑infarct patterns. Frequent mistakes include:
- Placing V1 and V2 too high, in the second or third intercostal space instead of the fourth.
- Misaligning V4–V6 so they are not on the same horizontal level.
- Swapping V1 and V2 or mislabeling chest lead positions on the cable.
- Using the nipple instead of anatomical landmarks to locate intercostal spaces, especially in female patients.
- Placing limb electrodes on the torso for a resting diagnostic ECG when standard practice calls for limb placement.
Training, checklists, and routine quality review of tracings are recommended to minimize lead placement errors.
How to Remember 12 Lead Placement

For younger children including infants, and those below 90lbs, ECG measuring via ribs isn’t usually applicable. Therefore, the pediatric 12 Lead ECG placement uses different placement angles for taking the necessary readings. Here is a detailed view of the pediatric 12 Lead ECG placement approach:
- V1: Placed on the nipple line to the right of the patient’s sternum.
- V2: Placed on the nipple line to the sternum’s left.
- V3: Stationed midway right between V2 and V4.
- V4: Placed on the midclavicular line right below the nipple.
- V5: Placed on the anterior axillary, which is at the same point as V4.
- V6: Placed just below the armpit at the midaxillary line (same as V4 and V5).
Quick Mnemonic and Checklist for 12 Lead ECG Placement
A simple checklist helps standardize placement, especially in busy clinical environments. Before recording, confirm the following:
- Patient relaxed, supine, skin clean and dry, hair clipped as needed.
- RA and LA on the distal arms; RL and LL on the legs above the ankles.
- V1 and V2 in the fourth intercostal spaces at the right and left sternal borders.
- V4 in the fifth intercostal space at the mid‑clavicular line; V3 between V2 and V4.
- V5 at the anterior axillary line; V6 at the mid‑axillary line, both level with V4.
Document any deviations from standard placement, such as torso limb leads for stress testing, on the ECG so that interpretation reflects the actual lead positions.
Frequently Asked Questions about 12 Lead ECG Placement
How many electrodes are used in a 12 lead ECG?
Where should limb leads be placed for a resting 12 lead ECG?
How do I find the correct position for V1 and V2?
What happens if chest leads are placed too high or too low?
Is lead placement different in female patients?
How is pediatric 12 lead ECG placement different from adult placement?
Can limb electrodes be placed on the torso?
What is Mason–Likar electrode placement?
How can I quickly check that my 12 lead ECG placement is correct?
Who should interpret a 12 lead ECG?
Need certified medical equipment or urgent technical support for your EKG systems?
Call Technical Support: (818) 362-7702At AIMCARDIO.COM we have a large variety of used EKG , refurbished EkG, and EKG machines. Please feel free to contact us today with any questions (818)362-7702